What is an Inframammary Fold or IMF
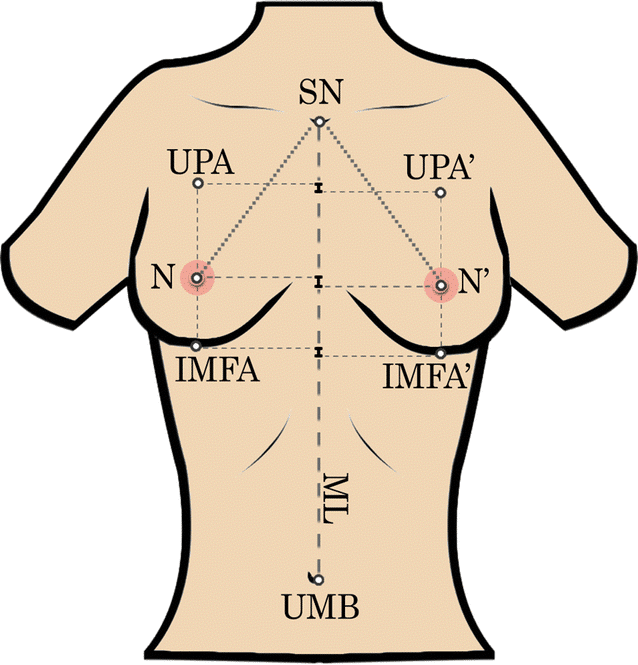
The inframammary fold (IMF) is the crease line where the lower part of the breast meets the chest wall. It serves as a natural boundary for breast augmentation procedures. It offers breast support while shaping and defining the overall breast shape and structure.
This structure is crucial to a woman’s breast anatomy and is vital for several breast surgery procedures. The inframammary fold defines the overall shape and structure and offers inferior support to the breast. Ideally, it is the depression defining the boundary between the chest wall and the breast, which is essential for a good bra fit.
The fold significantly affects the breast’s upper and lower pole, majorly the lower pole, influencing breast aesthetics before and after breast augmentation. Therefore, great care should be taken when performing breast surgery procedures, and the patient needs to understand the anatomy.
Due to its importance, understanding the inframammary fold should be one of the steps a patient takes before surgery. This article walks you through all the critical aspects regarding the inframammary fold, including the types, importance, related incisions, cases of malposition, and more to ease the hassle.
The Inframammary Fold – What Is It?
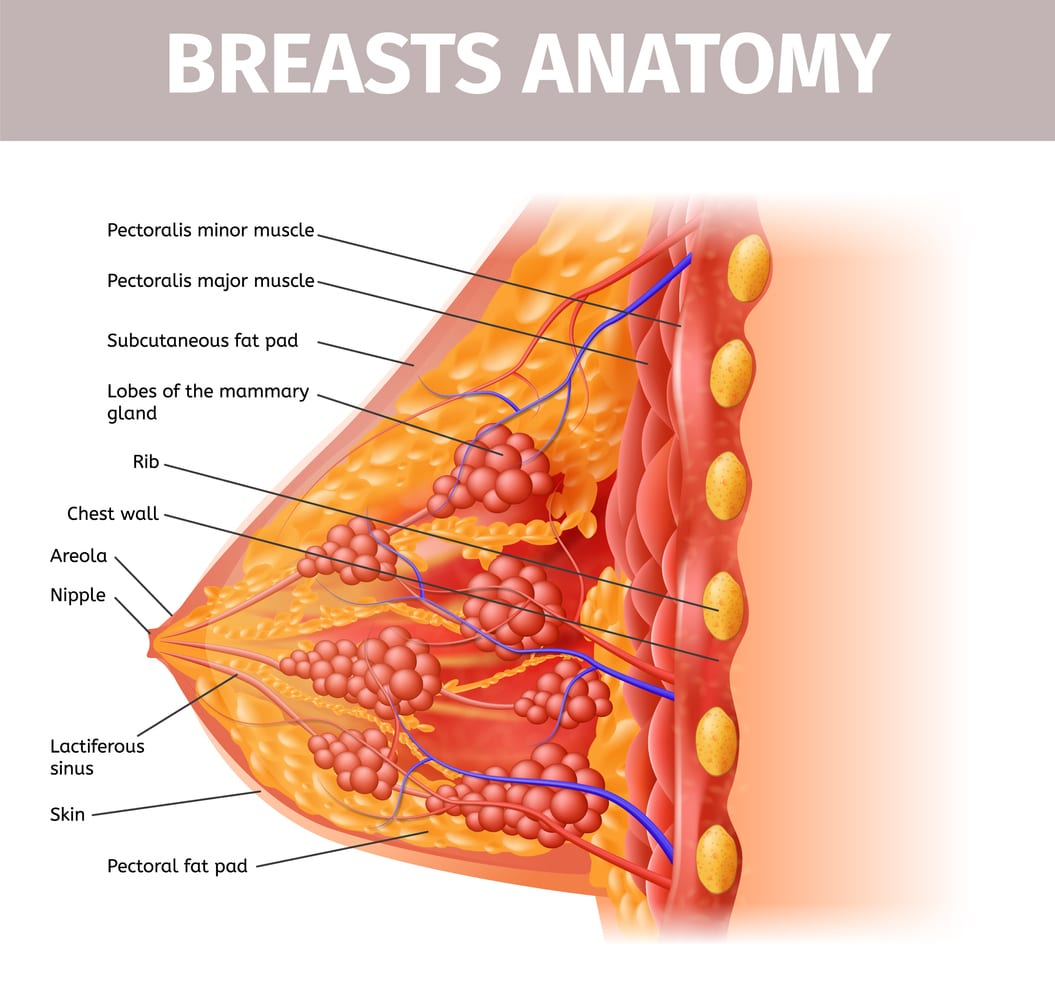
Breast Anatomy | BAA
The Inframammary fold is also known as the inframammary line or the inframammary crease. Despite most surgeons and medical researchers agreeing on the inframammary fold’s importance in breast augmentation procedure, there are discrepancies and controversies in theories explaining its anatomy. However, in simple terms, it’s the border where the lower pole of the breast meets the chest. The IMF is undetectable in a child up until puberty.
To describe the anatomy of the inframammary fold, one theory suggests that it is an inframammary ligament originating from the fifth to the sixth rib. The ligament then enters the dermis layer at the IMF level. Another theory shows that the formation of IMF mainly involves an increased collagen fiber density in the dermis.
The fibers offer support by attaching to the condensed superficial of the connective tissue. The other theory suggests the fold’s foundation constitutes dermal attachments to the deep and superficial fascia. It shows the fold as an osseo-fascia-cutaneous structure, with the key structure as the superficial fascia of the pectoralis major muscle.
Why should I care about the Inframammary fold?
The IMF holds significant importance both from a cosmetic and medical perspective in breast augmentation and reconstruction surgeries. Therefore, understanding and caring about the inframammary fold is essential. But why should you care about the fold? Let’s find out.
Cosmetic Significance

Some of the cosmetic significance include.
Symmetry between breasts
Achieving a symmetrical inframammary fold is crucial for creating a balanced and aesthetically pleasing appearance of the breasts. Surgeons typically aim for consistent and symmetrical folds to enhance the overall harmony of the breasts.
Matching fold to implant
Proper alignment of the inframammary fold with the breast implant is crucial for achieving harmonious results. When the fold is well-matched to the implant, it helps enhance the breast’s natural contours. Additionally, it ensures the nipple sits in an optimal position.
Reconstruction enhancement
In breast construction, creating a distinct and well-defined inframammary fold is vital for achieving a cosmetically pleasing result.
Medical Consideration
Double Bubble deformity
If the inframammary fold is not managed correctly during surgery, it can lead to a double bubble deformity. This occurs when the implant is positioned too high on the chest, creating a noticeable crease or indentation beneath the breast. The deformity can significantly affect the aesthetic outcome of the surgery.
Bottoming Out & Implant Displacement
This is another crucial thing to consider. Bottoming out is where the implant descends too low on the chest, causing an unnatural appearance. Ideally, bottoming out and implant displacement deformities can be avoided by using an anatomical approach during pocket dissection at IMF level. The surgeon should pay attention to the superficial pectoralis fascia when conducting the surgery for optimal results.
Poor Definition and Results
Neglecting the inframammary fold can result in poor breast definition and overall unsatisfactory surgical outcomes. A well-defined fold highly contributes to the breast’s shape and projection, ensuring a more successful surgery.
The above cosmetic and medical IMF significances are enough reasons to care about the inframammary fold.
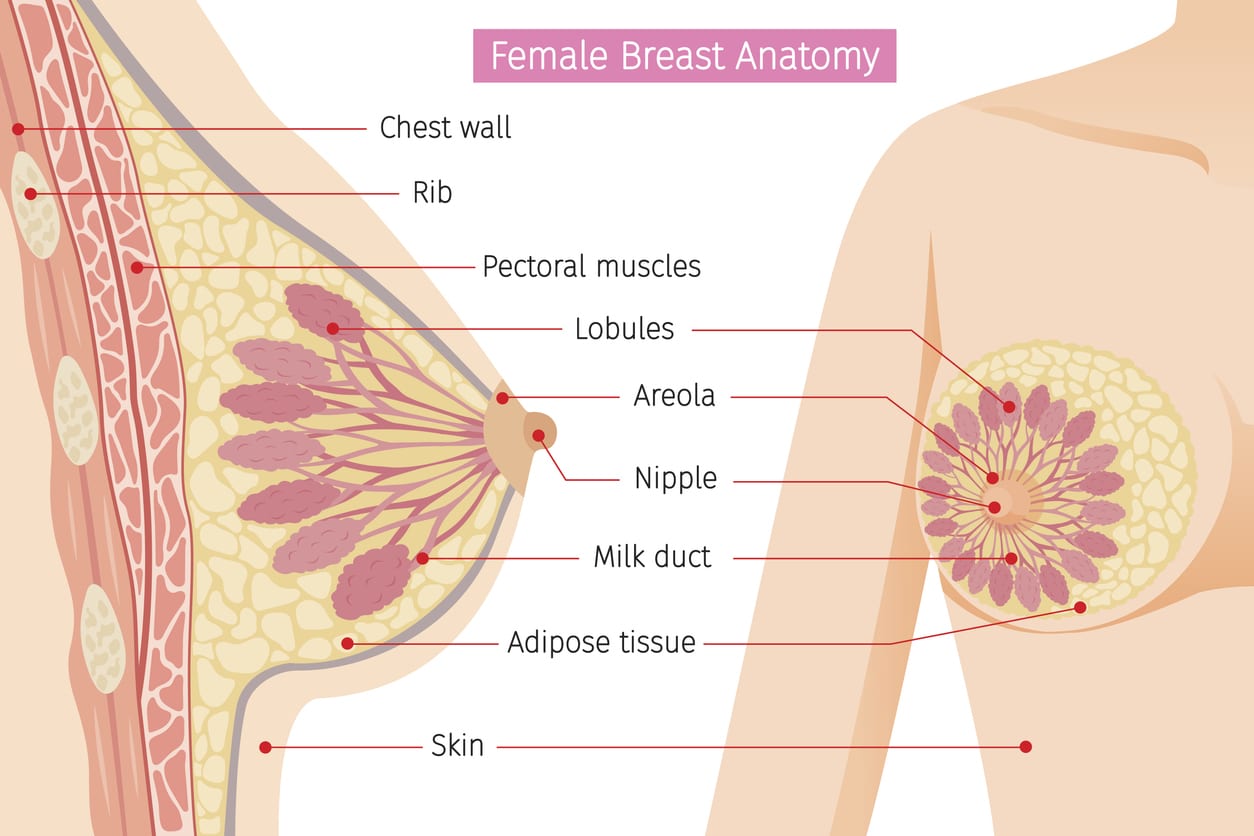
Understanding the Breast Anatomy
Every surgeon should understand and keenly consider the patient’s type of IMF and breast anatomy to advise them on the suitable breast surgery technique. Choosing the right specialist surgeon lowers the risk of post-surgical breast implant complications. It’s important to note that every patient is different regarding breast shape and size, and no technique suits all individuals. What does that tell you? The result may vary from one patient to the other.
Three tissues make up the breast: fat, connective, and glandular tissue. The glandular tissue consists of a network of ducts responsible for milk production, while the connective tissue holds all the tissues together and gives the breast shape. The fat tissue forms the adipose layer responsible for the breast size and contains the blood vessels and lymph nodes.
The breasts lay on the chest’s pectoral muscles, which are in two types: major and minor pectoralis muscle. The muscles are positioned above the ribs and covered by facia, a thin fibrous tissue layer. The muscles play a pivotal role in submuscular and dual plane placement techniques. The connective tissue comprises cooper ligaments that help keep the breasts perky and firm. Stretched cooper ligaments result in sagging breasts.
Patients with small breasts will have a small distance between the nipple and the inframammary fold. Therefore, if the surgeon doesn’t lower the IMF before creating a breast pocket, the incision’s scar will become visible on the breast. Lowering the fold allows room for breast enlargement and reduces the visibility of the incision’s scar.
Types of the Inframammary Folds
There are four different types of inframammary folds. The surgeon will conduct a test to determine the type of IMF and the kind of technique to use. The test mainly involves the patient raising their hands. Below are the types of IMF.
Type 0 IMF
The fold is almost non-existence and very hard to see. It allows the surgeon freedom to decide how they want to create the fold, where to start and end. The surgeon can decide to lower the fold.
Type 1 IMF
The fold disappears when the patient raises their hands. It’s only visible when the arms are by the side. It causes challenges during aesthetic breast surgery. Cohesive gel and advanced implant technology will help efface the fold.
Type 2 IMF
The fold is moderately prominent. However, it is only noticeable easily if the patient lifts their hands. The fold is there, but it’s less dominant. The surgeon can lower this type of fold but needs to be cautious by ensuring the lowering is minimum, less than 2cm. In addition, the surgeon may include performing fat grafting to enhance the results or customise the dual plane interface to ensure there’s no muscle covering it and the fold disappears completely.
Type 3 IMF
This fold is the hardest among the four. It looks like another typical fold but doesn’t disappear or change when the patient lifts their hands. Lowering the fold can be risky, and most surgeons prefer not to because errors can lead to a double bubble deformity.
Relationship of the IMF to Pectoralis Major Muscle
Knowledge of the correlation between pectoralis muscle and IMF positions can greatly influence surgical outcomes since both influence breast augmentation. Research indicates that the inframammary fold is inferior to the pectoralis major muscle inferior origin.
The dual plane technique involves creating a subpectoral pocket to the IMF, which results in the pectoralis major muscle release. Subpectoral dissection of the inframammary fold affects the pectoralis major muscle inferior origin.
Creating a subpectoral dissection to the IMF level will eliminate any inferior support offered by the pectoralis major muscle, leaving the IMF as the only inferior support to the implant. Therefore, the surgeon should make a judgment when lowering the fold because it eliminates the support the IMF offers, which can cause implant migration.
“High IMF, which can occur in women with tuberous breasts, short distance between the nipple and IMF, or constricted breasts, can result in shortened pectoralis major muscle. Therefore, as a FRACS specialist surgeon, I’m aware of the possible complications of submuscular placement in this group of patients.” Says Dr. Beldholm.
The Inframammary Incision
The inframammary incision is a standard technique surgeons use for different breast surgery procedures. It involves an incision along or underneath the inframammary fold. Some of the incision’s advantages include reduced visibility of scarring, direct visualisation of the implant pocket and breast tissue, and reusability during revision surgery.
Importance of the Inframammary Fold in Breast Surgery
The IMF plays an important role in different breast surgery procedures, including breast lift (mastopexy), breast reduction, breast augmentation, breast reconstruction, and breast revision.
Breast Augmentation
Inserting large breast implants can be challenging. However, an incision at the inframammary fold makes this possible, ensuring precision and minimal dissection of the breast tissue. It also reduces scar visibility and enhances recovery.
However, there should be an emphasis on IMF malposition. Surgeons can opt for the ‘Lucky 8’ stitch to ensure enhanced results. The technique involves inserting the needle through the rib periosteum at the IMF level, then piercing the lower part of the IMF incision from inside to outside. The next step is to pierce the incision’s upper part to form an 8 with the suture.
Breast Lift (Mastopexy)
Breast sagging (ptosis) can reduce the breasts’ aesthetics. Breast ptosis occurs in different degrees and will often require a breast lift to correct it. Surgeons use the inframammary line to assess the degree of breast ptosis. In normal breasts, the nipples and breast mound lie above the inframammary crease.
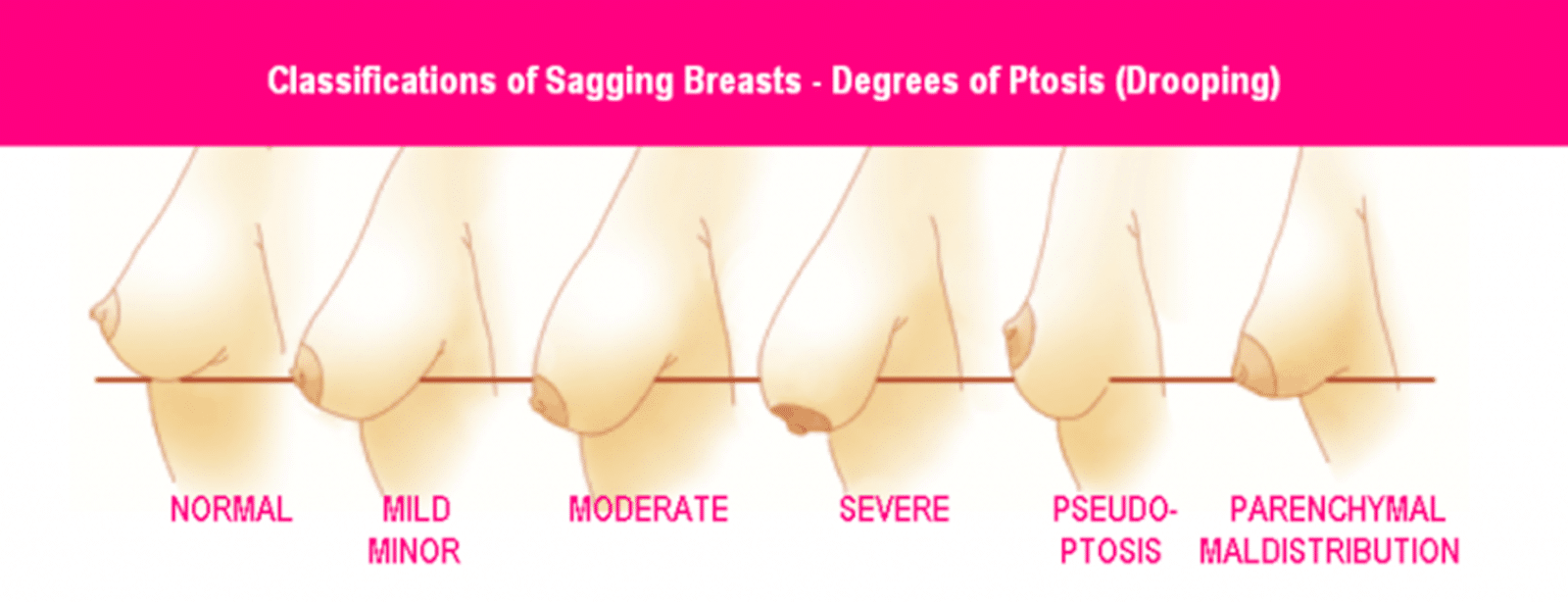
The different ptosis degrees include:
- Grade 1: This is mild ptosis, where the nipple is at the same level as the inframammary fold and above the breast contour.
- Grade 2: Mild ptosis where the nipple is below the inframammary fold but above the breast contour.
- Grade 3: Severe ptosis, where the nipple is below the inframammary fold and the breast contour.
- Pseudoptosis: Most of the breast mound is below the inframammary fold. However, the nipple is above it.
Breast Reduction
The procedure reduces the breast size, mostly in women suffering from chronic shoulder, back, or neck pain due to large breasts. Surgeons mostly carry out this procedure using inframammary fold techniques to enhance the results. The inframammary fold offers access to maximum tissue removal and reshaping.
One of the techniques is the Lolipop or vertical breast reduction. It involves one incision around the areola and another vertical, running from the areola to the inframammary line. The other technique is the Anchor or inverted-T breast reduction. It involves making two incisions vertically from the areola to the inframammary line and along the inframammary fold. There’s also a third incision around the areola.
Breast Revision
Revision surgery involves the removal and replacement of a breast implant. Many women undergo the procedure to change the implant type and size or due to complications like BIA-ALCL, capsular contracture, and malposition.
Implant malposition can result from over-dissection of the inframammary fold when creating the implant pocket. To correct the complication, the surgeon can use the capsulorrhaphy technique to reduce the implant pocket size.
Reconstruction of the Inframammary Fold
Inframammary fold reconstruction is one of the most complex surgical procedures. Despite several reconstruction techniques, no method produces results similar to a normal breast’s IMF. Therefore, surgeons should try to preserve the inframammary fold during breast surgery procedures like mastectomy. Preservation of the inframammary fold during mastectomy facilitates breast reconstruction. Therefore, most surgeons practice IMF conservation during mastectomy, contrary to the previous total mastectomy.
The surgeon often requires a large incision during reconstruction, which may increase surgical invasiveness. Some techniques used in inframammary reconstruction include sutures, fascial flaps, drawstring method, and adipofascial flaps. The type of technique will depend on the patient’s breast anatomy, the type of breast implants, and the surgeon’s advice.
IMF Low Positioning?
Lowering the IMF during breast enlargement is a common practice. However, there are instances when excessive fold lowering may result in a downward implant displacement with the nipples tilted upwards. Low IMF positioning can cause a double bubble.
IMF High Positioning?
When positioning the IMF, the surgeon may raise the IMF too high, resulting in high-riding breasts. If the surgeon positions the IMF at the nipple’s level or higher, it can result in upper breast fullness and a downward-pointing nipple.
Bottom Line
The inframammary fold is an important breast structure, vital in several breast surgery procedures. Therefore, patients should understand its importance before breast surgery to discuss different surgical techniques with plastic surgeons. Preserving the IMF should be key in any surgical procedure to reduce the need for IMF reconstruction, which can be challenging.
References
- Atiyeh, B. S., Ibrahim, A. M. H., Saba, S. C., Karamanoukian, R. L., Chahine, F., & Papazian, N. (2017). The Inframammary Fold (IMF): A Poorly Appreciated Landmark in Prosthetic/Alloplastic Breast Aesthetic and Reconstructive Surgery—Personal Experience. Aesthetic Plastic Surgery, 41(4), 806–814.
- Tomita, K., Taminato, M., Nomori, M., Maeda, D., Seike, S., Tashima, H., Yano, K., & Kubo, T. (2020). A Simple and Scarless Method for Inframammary Fold Correction Using a Barbed Suture. Plastic and Reconstructive Surgery. Global Open, 8(6), e2930.
- Ono, M. T., & Karner, B. M. (2019). Four-step Augmentation Mastopexy. Plastic and Reconstructive Surgery. Global Open, 7(11), e2523.
- Brown, M. H., Shenker, R. L., & Silver, S. A. (2005). Cohesive Silicone Gel Breast Implants in Aesthetic and Reconstructive Breast Surgery. Plastic and Reconstructive Surgery, 116(3), 768–779.
- Campbell, C. F., Small, K., & Adams, W. M. (2015). The Inframammary Fold (IMF) Fixation Suture: Proactive Control of the IMF in Primary Breast Augmentation. Aesthetic Surgery Journal, 36(5), 619–623.
- Nanigian, B. R., Wong, G. B., & Khatri, V. P. (2007). Inframammary crease: Positional relationship to the pectoralis major muscle origin. Aesthetic Surgery Journal, 27(5), 509–512.
- Cannistrà, C., Trivisonno, A., Deschler, A., Aboud, C., Shiffman, M. A., & Monti, M. (2018). A Simple Algorithm for the Inframammary Fold Reconstruction, Balcony-Like Technique. The American Journal of Cosmetic Surgery.
- Atiyeh, B. S., Ibrahim, A. M. H., Saba, S. C., Karamanoukian, R. L., Chahine, F., & Papazian, N. (2017b). The Inframammary Fold (IMF): A Poorly Appreciated Landmark in Prosthetic/Alloplastic Breast Aesthetic and Reconstructive Surgery—Personal Experience. Aesthetic Plastic Surgery, 41(4), 806–814.
- Gui, G., Behranwala, K. A., Abdullah, N., Seet, J., Osin, P., Nerurkar, A., & Lakhani, S. R. (2004). The inframammary fold: contents, clinical significance and implications for immediate breast reconstruction. British Journal of Plastic Surgery, 57(2), 146–149.
- Maclin, M. M., Deigni, O. A., & Bengtson, B. P. (2015). The laminated nature of the pectoralis major muscle and the redefinition of the inframammary fold. Clinics in Plastic Surgery, 42(4), 465–479.
- Ouyang, Y., Du, X., Ma, X., Fu, A., & Liu, C. (2021). Prevention and Management of Double-Bubble Deformity in augmentation Mammoplasty. Aesthetic Plastic Surgery, 46(S1), 85–86.
- Handel, N. (2013). The Double-Bubble deformity. Plastic and Reconstructive Surgery, 132(6), 1434–1443.
- Massiha, H. (2000). Augmentation in ptotic and densely glandular breasts: Prevention, treatment, and classification of double-bubble deformity. Annals of Plastic Surgery, 44(2), 143–146.
- Salgarello, M., & Visconti, G. (2017). Staying out of Double-Bubble and Bottoming-Out Deformities in Dual-Plane breast augmentation: Anatomical and Clinical study. Aesthetic Plastic Surgery, 41(5), 999–1006.
- Tebbetts, J. B. (2006). Dual plane breast augmentation: optimizing Implant-Soft-Tissue relationships in a wide range of breast types. Plastic and Reconstructive Surgery, 118(Supplement), 81S-98S.
- Benito-Ruiz, J. (2023). The position of the Nipple-Areola complex in breast augmentation. Aesthetic Surgery Journal.
- Montemurro, P., Otte, M. S., Wagner, J. M., Pafitanis, G., Cheema, M., & Hedén, P. (2023). Anatomical variations of the pectoralis muscle and its importance for breast implant surgery. Plastic and Reconstructive Surgery. Global Open, 11(1), e4761.
- Weniger, F. G., Barrero, C. E., Weidman, A. A., & Amarillo, S. M. (2021). Factors Affecting Lower-pole Stretch after Breast Augmentation. Plastic and Reconstructive Surgery. Global Open, 9(11), e3865.
- Atiye, B., & Chahine, F. (2018). Metrics of the aesthetically perfect breast. Aesthetic Plastic Surgery, 42(5), 1187–1194.
- Kraft, C. T., Rendon, J. L., Koutz, C. A., & Miller, M. J. (2019). Inframammary fold reconstruction in the previously reconstructed breast. Plastic and Reconstructive Surgery, 143(4), 1019–1029.



