What is a Dual Plane Technique
Choosing the implant pocket location and the placement technique for a breast augmentation procedure is crucial before surgery.
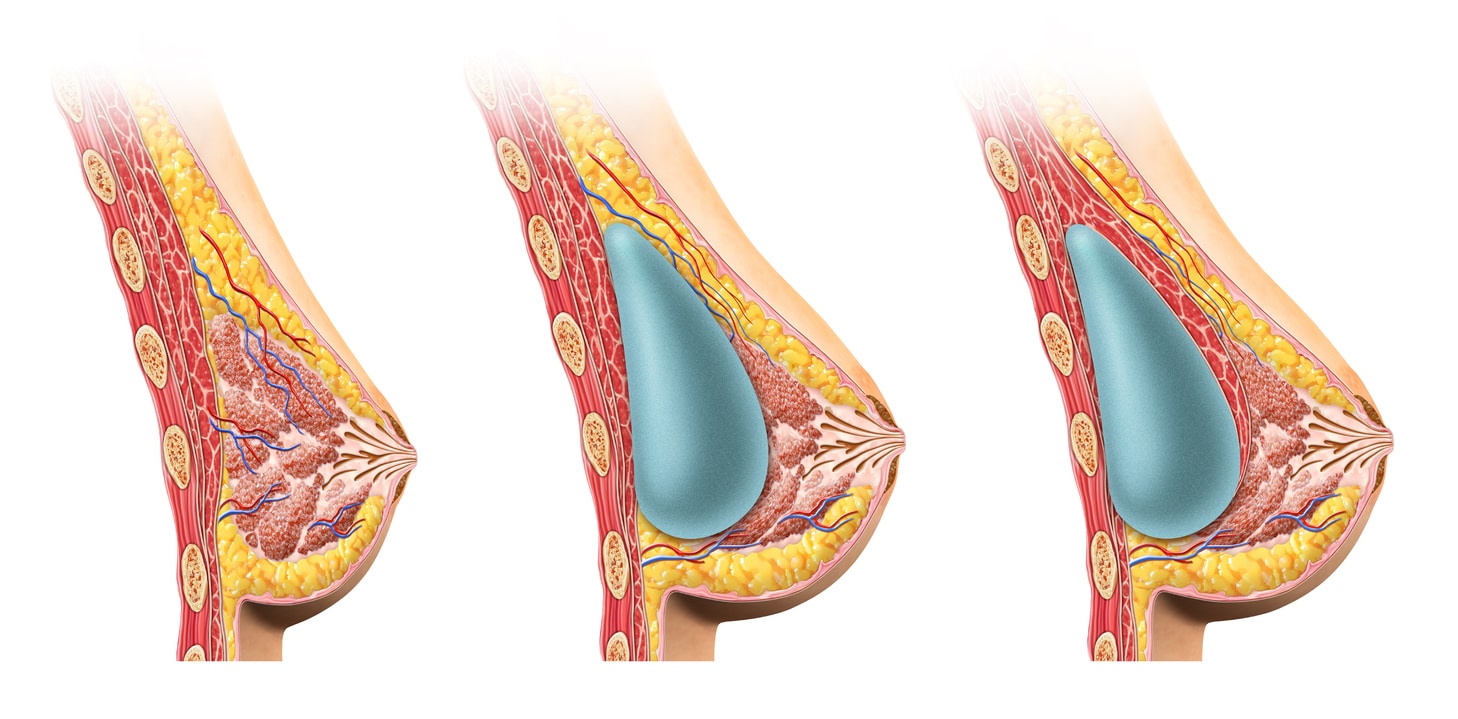
In the dual plane technique, the surgeon places the breast implant partially behind the pectoralis major muscle and partially behind the breast parenchyma. Therefore, the implant is in dual planes simultaneously; the implant’s upper part is under the muscle, while the lower part is under the breast gland.
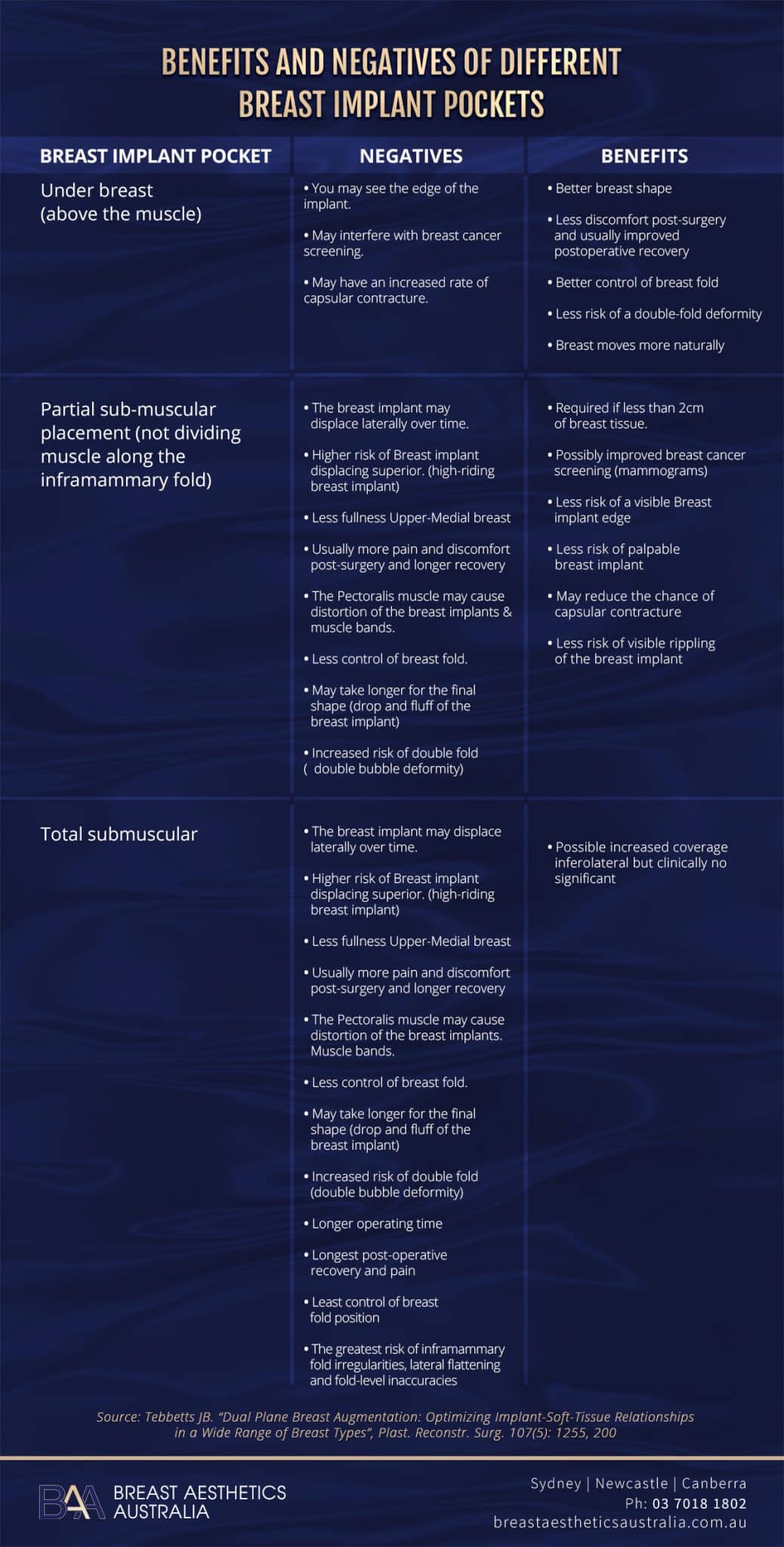
The placement technique largely influences the final aesthetic appearance of the breasts. Mostly, the pocket locations are either total submuscular (totally behind the pectoralis major muscle and serratus), partial retropectoral (partially behind the pectoralis major muscle), or retromammary (behind breast parenchyma)
Each pocket location poses different advantages and disadvantages. The dual plane breast augmentation technique minimises the downsides of single pocket location, especially under the muscle implant placement. Let’s dive deeper into this topic and learn more.

What is a Dual Plane Breast Augmentation Placement Technique?
Unlike the standard single pocket location placement methods, the dual plane implant placement utilises dual planes simultaneously. The breast implant is partially behind the pectoralis major muscle and partially behind the breast gland.
The dual plane technique can also involve total division of the origin of a specific pectoralis muscle group to change implant-soft tissue dynamics. The plastic surgeon does this by anatomically repositioning the pectoralis major muscle portions relative to the breast implant. This factor distinguishes partial retropectoral augmentation and dual plane.
In addition, the dual plane technique can involve the alteration of the parenchyma-muscle interface. This changes the soft tissue relationships between the parenchyma and pectoralis major muscle and the implant-parenchyma dynamics.
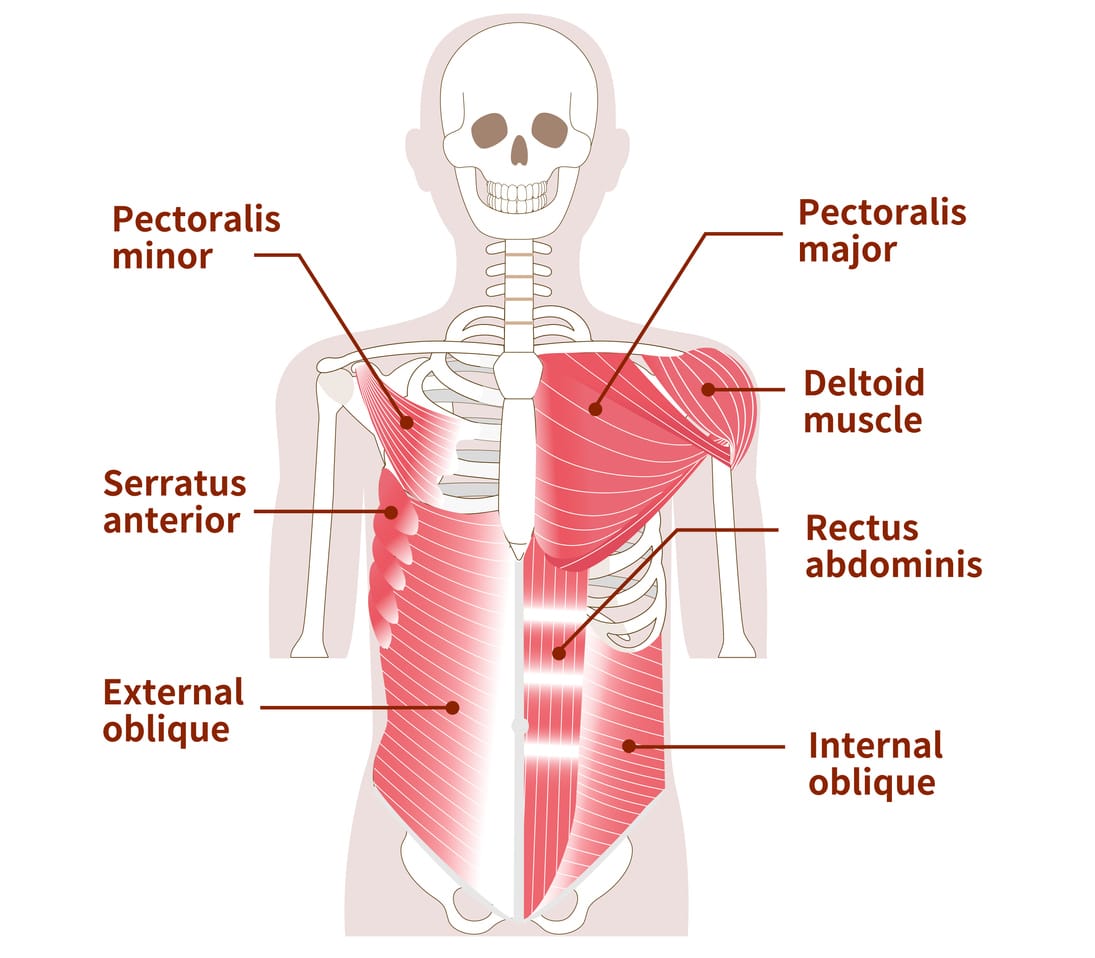
Several factors control the pectoralis major muscle relation to the breast implant. These are the origins of the pectoralis muscle along the sternum medially and the inframammary fold inferiorly, and the pectoralis attachments to the breast parenchyma found at the parenchyma-muscle interface. Depending on the tissue characteristics, incisional approach, and breast type, the surgeon makes incisions on these two to different degrees.
In the dual plane technique, the pectoralis major muscle covers part of the breast implant while the breast tissue covers the other part.
“The part of the implant covered by the breast tissue settles into a natural breast shape and feel because of the smooth implant-breast transition. However, it may take longer to achieve the final results as the breast tissue heals, allowing the implant to settle.” Says Dr. Beldholm.
The pectoralis major muscle covering the upper part reduces the risk of synmastia, capsular contracture, implant visibility, and rippling. It also helps improve mammography accuracy.
What are the Different Types of Dual Plane Techniques?
Three different types of dual-plane breast augmentation techniques exist, depending on the degree of muscle division and parenchyma-muscle interface dissection. The pectoralis major muscle is attached to the ribs and the sternum, and it’s what is adjusted. The sternal part is never detached. The dual plane technique variations are type 1, type 2, and type 3.
Dual Plane Technique Type 1
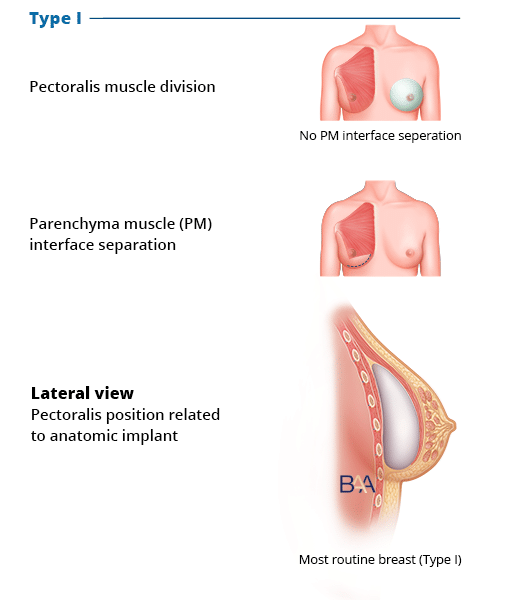
Tebbetts dual plane Type 1 | BAA
In this type, the surgeon completely divides the pectoralis origins across the inframammary fold up to the inframammary fold medial aspect. Most plastic surgeons don’t dissect the retromammary plane, which would free the parenchyma-muscle interface.
The division detaches the lower fibres of the pectoralis muscle, causing the muscle to rise a little but stay attached to the overlying breast tissue. The pectoral muscle covers most of the breast implant, leaving only a small lower portion.
Dual Plane Technique Type 2
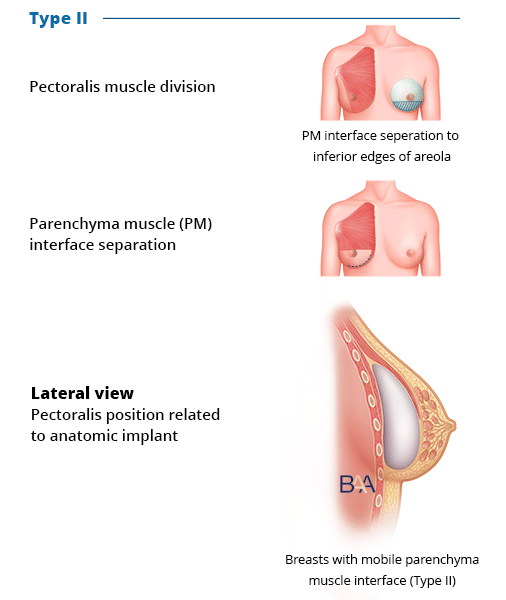
Tebbetts dual plane Type 2 | BAA
In addition to the complete division of the pectoralis origins across the inframammary fold up to the inframammary fold medial aspect, the surgeon dissects the retromammary plane. The dissection reaches up to the lower areola border.
The breast tissue covers the lower portion of the implant, improving slight breast sagging and reducing the risk of a dynamic double bubble. It’s suitable for patients aiming to improve their breast shape and size.
Dual Plane Technique Type 3
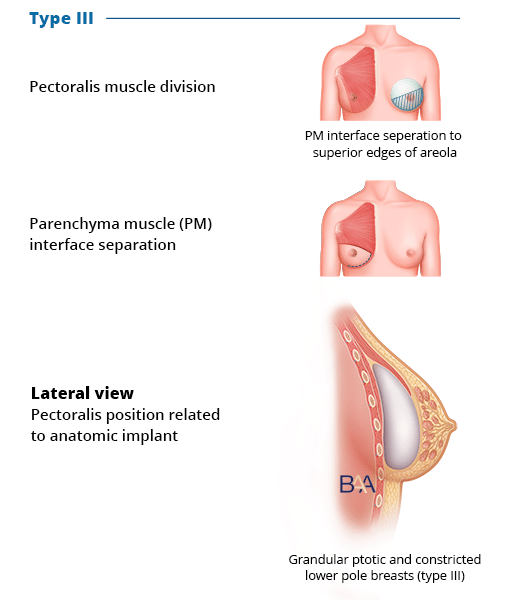
Tebbetts dual plane Type 3 | BAA
This technique is like the type 2 dual plane approach. However, in type 3, the surgeon makes the dissection in the retromammary plane a little higher, around the areola superior border.
The dissection expands the breast’s lower portion more than in type 2. This helps elevate the areola and nipple, improving the appearance of mild sagging without breast lift surgery (mastopexy).
 Who is Best Suited for Dual Plane Technique?
Who is Best Suited for Dual Plane Technique?
The dual plane technique is considered advantageous for implant placement, but it may be more suitable for certain individuals, such as women with thin natural breast tissue.
This technique provides better muscle coverage around the implant’s upper area, reducing the need for breast tissue coverage, and can also correct mild breast ptosis caused by breastfeeding, weight loss, age, or pregnancy.
It is also effective for women with tuberous breasts as it expands the lower pole and corrects downward-facing nipples, resulting in a more attractive shape.
What Holds the Breast Implant in Dual Plane Placement Technique?
When the surgeon inserts the breast implant into the pocket, it exerts pressure on the breast’s lower pole, causing the breast skin to stretch. The supporting tissue around the inframammary fold holds the implant in place, reducing the bottoming-out risk. Therefore, the surgeon should ensure the dissection is above the inframammary fold. In addition, it should not cut the fold attachments to the chest wall.
Does the Dual Plane Technique Eliminate the Need for Mastopexy?
Mastopexy (breast lift) is a procedure to correct breast sagging (ptosis). As the breast implant settles in the pocket, it causes the breast’s lower pole to expand and fill out, giving a lifted appearance. It can also raise the nipple/areola position. This treats mild breast sagging.
However, dual plane breast augmentation doesn’t eliminate the need for mastopexy since it cannot correct a higher degree of breast sagging. The patient must undergo mastopexy to correct breast ptosis and achieve long-term results.
Exercising After Dual Plane Technique

Undergoing dual plane breast augmentation doesn’t prevent the patient from exercising. However, the strength of the pectoral muscle is reduced, especially in type 2 and 3 techniques, which may affect exercising in the first few days. With time, the patient gradually eases into normal exercising.
Pros of Dual Plane Technique
There are several advantages that come with dual plane technique. Let’s have a closer look at them.
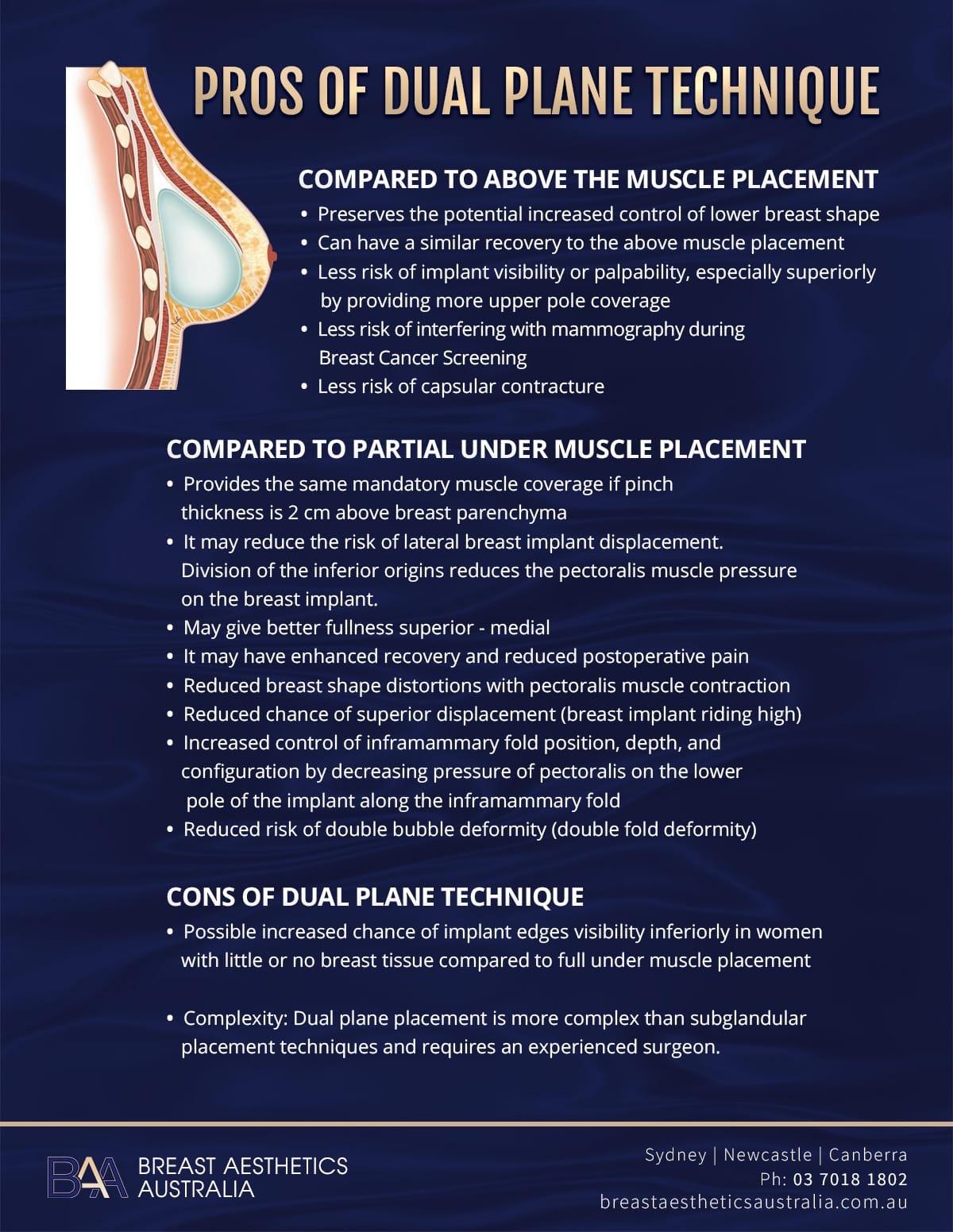
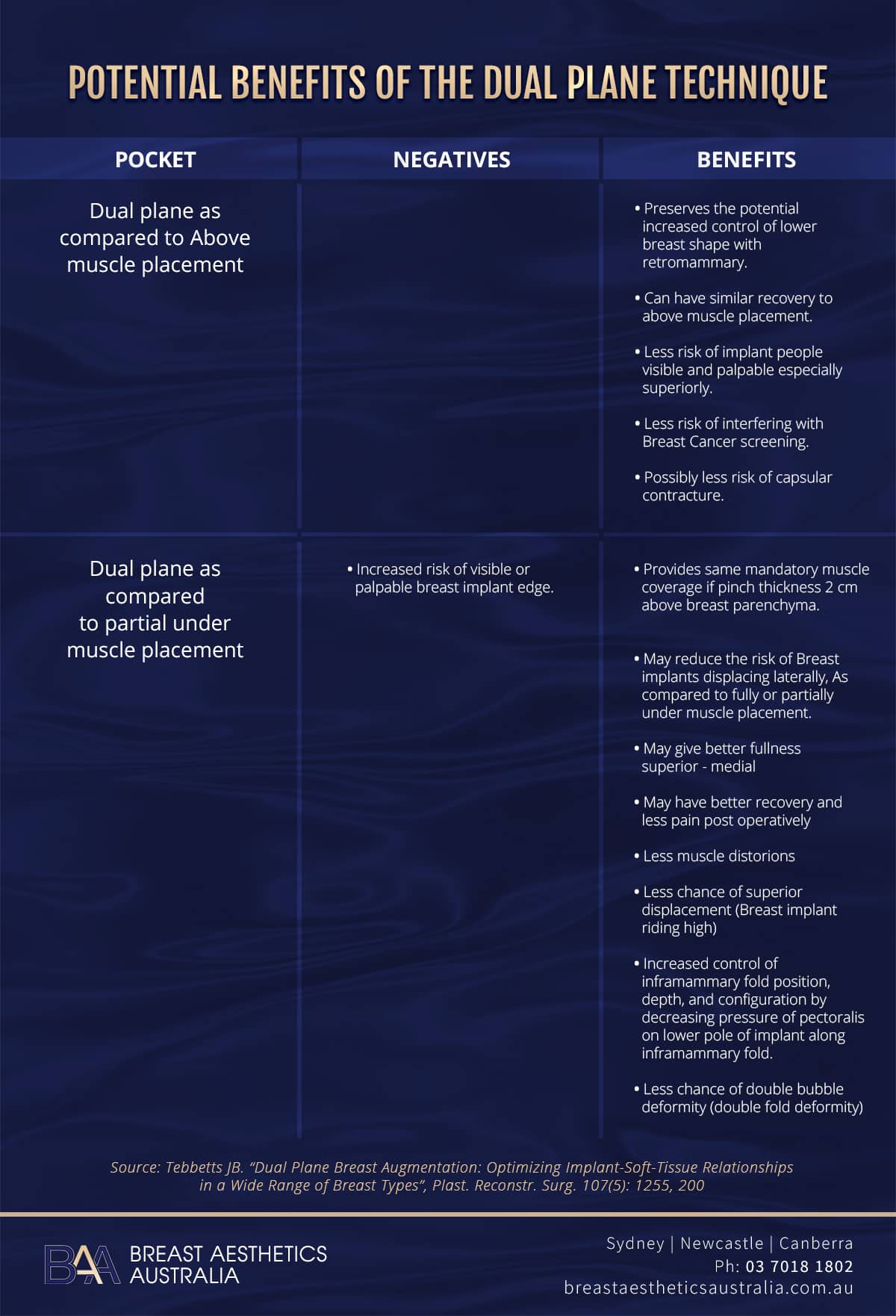
Compared to Above the Muscle Placement
- Preserves the potential increased control of lower breast shape
- Can have a similar recovery to the above muscle placement
- Less risk of implant visibility or palpability, especially superiorly by providing more upper pole coverage
- Less risk of interfering with mammography during Breast Cancer Screening
- Less risk of capsular contracture
Compared to Partial Under Muscle Placement
- Provides the same mandatory muscle coverage if pinch thickness is 2 cm above breast parenchyma
- It may reduce the risk of lateral breast implant displacement. Division of the inferior origins reduces the pectoralis muscle pressure on the breast implant.
- May give better fullness superior – medial
- It may have enhanced recovery and reduced postoperative pain
- Reduced breast shape distortions with pectoralis muscle contraction
- Reduced chance of superior displacement (breast implant riding high)
- Increased control of inframammary fold position, depth, and configuration by decreasing pressure of pectoralis on the lower pole of the implant along the inframammary fold
- Reduced risk of double bubble deformity (double fold deformity)
Cons of Dual Plane Technique
- Possible increased chance of implant edges visibility inferiorly in women with little or no breast tissue compared to full under muscle placement
- Complexity: Dual plane placement is more complex than subglandular placement techniques and requires an experienced surgeon.
Other Implant Placement Techniques
There are other placement techniques besides the dual plane technique. The techniques include partial subpectoral, where the breast implant is partially under the pectoralis muscle; subfascial, where the breast implant is under the fascia and breast glands covering the pectoral muscle but over the muscle; submuscular, and subglandular. The last two placement techniques are widely used.
Subglandular Placement Technique
The technique involves the placement of the breast implant above the muscle but behind the breast tissue. Subglandular technique is less invasive than submuscular and can result in less healing period, reduced risk of lateral malposition, and breast animation.
It doesn’t affect the chest muscles and leads to a bigger cleavage because the breast implants are close together. The technique can also accommodate large breast implants. However, it can cause future breastfeeding problems and interfere with mammography tests. In addition, the subglandular technique can result in the following:
- Loss of nipple sensation,
- Less natural look
- Increased bottoming out risk
- Capsular contracture
The subglandular placement technique is suitable for patients with a high amount of existing breast tissue to cover the implant. This makes the technique less suitable for patients with thin breast tissue because it increases the risk of visible implant edges and rippling.
 Submuscular Placement Technique
Submuscular Placement Technique
The submuscular implant placement technique involves the placement of the breast implant behind the pectoral muscle. It holds the implant in place, reducing movement and the risk of capsular contracture. The placement provides a natural look and reduces the risk of implant visibility and inferior malposition. In addition, it doesn’t affect the accuracy of future mammography tests. However, the procedure may have a longer recovery period due to manipulation of the chest muscle, and there’s visible animation during physical exercise.
The technique is suitable for patients with little breast tissue because it enhances the breast shape while reducing implant visibility and rippling. In addition, it’s suitable for patients undergoing a breast lift (mastopexy) because it optimises blood flow.
Which is the Right Implant Placement Option?

You may be confused about the right placement technique for breast implant procedures between dual plane, submuscular, or subglandular. The best thing is to consult your surgeon before settling for one technique. The surgeon will advise you on the suitable implant placement technique.
The technique’s suitability will depend on the existing breast tissue, desired aesthetics, and body type. Your medical history and the type of breast implant also determine the suitability of a specific technique for breast augmentation surgery.
It’s important to note that no breast implant placement technique suits everyone equally. Different techniques will suit various women, and the final results may vary from the desired or expected results.
Dr. Beldholm notes, “The best results with the best recovery tend to be breast implants placement above the muscle. This allows the implants to move more naturally, avoiding muscle bands and displacement. However, if the breast tissue is too thin for this technique, a dual plane can be a great alternative with many benefits.”
Bottom Line
The dual plane changes the relationship between the breast tissue and the pectoralis major muscle, minimising disadvantages posed by placing the breast implants under the muscle. It advances subglandular and submuscular placement techniques. The dual plane technique leads to more natural-looking breasts and reduces the risks of post-surgical complications.
However, the placement technique is only suitable for some, and patients should consult with a specialist surgeon to determine their suitability. If you’re looking for breast augmentation in Newcastle, Sydney or Canberra, contact us for customised breast augmentations.
References
- Tebbetts, J. B. (2001). Dual Plane Breast Augmentation: Optimising Implant-Soft-Tissue Relationships in a Wide Range of Breast Types. Plastic and Reconstructive Surgery, 107(5), 1255–1272.
- Karabeg, R., Jakirlic, M., Karabeg, A., Crnogorac, D., & Aslani, I. (2019a). The New Method of Pocket Forming for Breast Implant Placement in Augmentation Mammaplasty: Dual Plane Subfascial. Medicinski Arhiv, 73(3), 178.
- Bekisz, J. M., Salibian, A. A., Frey, J. D., Choi, M., & Karp, N. S. (2022). Picking the Right Plane: A Comparison of Total Submuscular, Dual-Plane, and Prepectoral Implant–Based Breast Reconstruction. Plastic and Reconstructive Surgery, 150(4), 737e–746e.
- Hwang, D. S., Park, S. M., & Kim, S. H. (2017). A Modified Dual-plane Technique Using the Serratus Anterior Fascia in Primary Breast Augmentation. Plastic and Reconstructive Surgery. Global Open.
- Graf, R., Bernardes, A., Rippel, R., Araujo, L. H., Damasio, R. C. C., & Auersvald, A. (2003). Subfascial Breast Implant: A New Procedure. Plastic and Reconstructive Surgery, 111(2), 904–908.
- Vázquez, B., Ks, G., & Houston, G. C. (1987b). Breast augmentation: A review of subglandular and submuscular implantation. Aesthetic Plastic Surgery, 11(1), 101–105.
- Maluf, I., Junior, Graf, R., Ascenço, A. S. K., Itikawa, W. M., Balbinot, P., Munhoz, A. M., Lopes, M. S., Nasser, I. J. G., Urban, L. a. B. D., & Da Silva Freitas, R. (2019). Is There a Breast Augmentation Outcome Difference Between Subfascial and Subglandular Implant Placement? A Prospective Randomized Double-Blinded Study. Aesthetic Plastic Surgery, 43(6), 1429–1436.
- Headon, H., Kasem, A., & Mokbel, K. (2015d). Capsular Contracture after Breast Augmentation: An Update for Clinical Practice. Archives of Plastic Surgery, 42(05), 532–543.
- Qureshi, A. G., Myckatyn, T. M., & Tenenbaum, M. M. (2018). Mastopexy and Mastopexy-Augmentation. Aesthetic Surgery Journal, 38(4), 374–384.